Toothache or tooth pain is caused when the nerve root of a tooth is irritated. Dental
(tooth) infection, decay, injury, or loss of a tooth are the most common causes
of dental pain.
The first step in the evaluation of oral pain should be to determine its aetiology.
Dental sources are most common. However, pain arising from non-dental sources such
as myofascial inflammation, migraine, maxillary sinusitis, nasal tissues, ears,
temporomandibular joints, anginas and neuralgias always must be considered and excluded.
Caries is initially asymptomatic. Pain does not occur until the decay impinges on
the pulp, and an inflammatory process develops.
Reversible pulpitis is characterised by pain caused by stimuli such as cold. It
usually does not last for very long, and usually stops on removing the stimuli.
If left untreated it can progress to irreversible pulpitis.
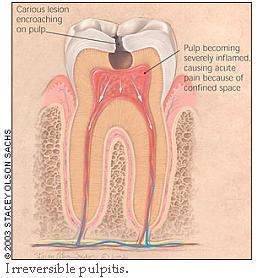
Irreversible Pulpitis
Figure 1: Carious lesion
If a carious lesion causing reversible pulpitis is not treated, the condition will
progress to irreversible pulpitis, a severe inflammation of the pulp (Figure 1).
Signs and Symptoms
Pain becomes severe, spontaneous, and persistent, and is often poorly localized.
Patient may complain of pain with hot foods and liquids.
Pain during recumbence
and even spontaneous pain.
Management
The only way to definitively treat the discomfort is root canal treatment (removal
of the pulp and filling of the empty pulp chamber and canal) or extraction of the
tooth.
The pain should be managed with appropriate analgesia such as a non-steroidal
anti-inflammatory drug (NSAID) or a weak opioid combined with an NSAID or acetaminophen.
Patients should be warned of the risks of further complications if they do not have
prompt definitive treatment.
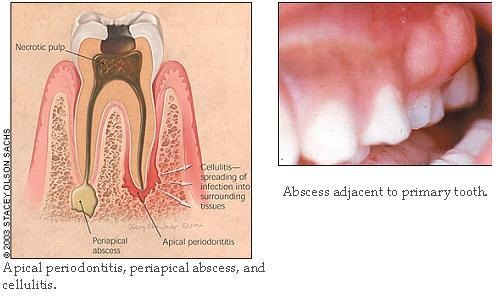
Apical Periodontitis
A severely inflamed pulp will eventually undergo necrosis, causing apical periodontitis,
which is inflammation around the apex of the tooth (figure 2).
Signs and Symptoms
Pain is severe, spontaneous, persistent and localizes to the affected tooth.
The tooth is sensitive to percussion with a metal object.
Regional lymphadenopathy
can be present.
Management
Root canal treatment or extraction.
Figure 2 and 3: Apical Abscess
Apical Abscess
Apical abscess is a localized, purulent form of apical periodontitis (Figures 2
and 3).
Signs and Symptoms
It may present clinically as a fluctuant buccal or palatal swelling, with or without
a draining fistula.
Regional adenopathy is usually present.
If pus is draining, pain usually is not severe.
Management
Antibiotics are not necessary unless concurrent cellulitis is present.
Acute
incision and drainage of the fluctuant area results in immediate relief to the patient
Definitive therapy is root canal treatment or extraction.
Cellulitis
Cellulitis may follow apical periodontitis if the infection spreads into the surrounding
tissues(Figure 2).
Signs and Symptoms
Diffuse, tense, painful swelling of the affected tissues occurs.
Regional
lymphadenopathy is common, and fever may be present.
The infection can spread
into the major fascial spaces of the head and neck, with the attendant risk of
airway compromise.
Maxillary infection also may spread to the periorbital area,
increasing the risk of serious complications that include loss of vision, cavernous
sinus thrombosis, and central nervous system involvement.
Management
The examination should focus on determining if the cellulitis remains localized
or has spread regionally.
Patients with localized cellulitis are treated with
antistreptococcal oral antibiotics, such as oral penicillin in a dosage of 500 mg
three times daily in adults or 50 mg per kg per day divided into three doses in
children.
In the event of true penicillin allergy, erythromycin or clindamycin may be substituted.
Appropriate pain medication should be provided.
Definitive therapy is root canal treatment or extraction, which in selected cases
may be delayed until swelling has subsided.
If infection extends regionally into the deep spaces of the head and neck as evidenced
by severe swelling, the risk of life-threatening complications such as airway compromise
is substantial.
Generally, these patients should be hospitalized and provided with surgical and
infectious disease consultation. Imaging, usually with computed tomographic scanning,
is mandatory, as is surgical drainage if abscess formation is detected.
Intravenous
broad-spectrum antibiotic treatment should be started immediately and should include
coverage for anaerobes.
Paediatric Considerations
In general, the same principles of initial evaluation and management apply to the
primary and permanent dentition. However, carious lesions of the primary teeth less
frequently cause pain and abscesses and more frequently drain cutaneously than lesions
of the permanent dentition. The systemic effects of infection are more pronounced
in children, with rapid temperature elevations, greater risk of dehydration, and
more rapid spread of infection.
Periodontal disease is an inflammatory destruction of the periodontal ligament and
supporting alveolar bone. The main etiologic agent is bacterial plaque. Multiple
bacteria are implicated, but as the disease progresses, gram-negative anaerobes
predominate.
Acute Periodontal Abscess
Patients with chronic periodontal disease or patients who have a foreign object
lodged in the gingiva may present with an acute periodontal abscess.
Signs and Symptoms
Throbbing pain with erythema and swelling over the affected tissue.
The tooth is normally tender to percussion and shows increased mobility.
Management
If left untreated, the abscess may rupture or, less commonly, progress to cellulitis.
Within 24 hours drainage and debridement of the infected periodontal area must be
done.
Antibiotics are not normally indicated if debridement is successful, but they may
be used depending upon the dentists discretion.
Pericoronitis is inflammation of the soft tissues surrounding the crown of a partially
erupted tooth, most commonly a wisdom tooth (Figure 4). It occurs when bacterial
plaque and food debris accumulate beneath the flap of gum covering the partially
erupted tooth.
Signs and Symptoms
Inflammatory oedema, often complicated by trauma from the opposing tooth, leads
to swelling of the flap, pain and tenderness.
Bad taste caused by pus oozing from beneath the flap.
Regional lymphadenopathy is common, and cellulitis and trismus (inability to open
the mouth fully) can occur.
In severe cases, the oral airway can be compromised.
Figure 4: Pericoronitis
Management
If pericoronitis is well localized, hot salty mouthwashes and irrigation under the
flap can resolve symptoms in the majority of cases.
Localized cases that do
not respond to mechanical therapy and more severe disseminated cases with spreading
cellulitis should be treated with penicillin and appropriate pain medication.
The patient should be evaluated to see if symptomatic treatment can suffice until
eruption is complete or if surgical therapy to remove the gum flap or underlying
tooth is necessary.
Dental Trauma
Dental trauma is extremely common. Children are particularly affected, with one
third of five year olds having suffered injury to their primary teeth, and one fourth
of 12 year olds having suffered injury to their permanent teeth. Injuries to teeth
and their supporting structures can be classified as fractures, lateral or extrusive
luxation (loosening and displacement of the tooth), intrusion (displacement of the
tooth vertically into the alveolar bone), and avulsion (complete displacement of
the tooth out of its socket).
The mechanism of injury and timeline are particularly important aspects of the history
because they define the risk of associated injuries and available treatment options.
Examination should focus on related soft tissue injuries and the need for suturing,
signs of tooth loosening, displacement or fracture, and disturbance in the bite
or other signs of alveolar fracture. Complete diagnosis requires at least one dental
radiograph in all cases.
All patients with traumatized teeth ultimately need follow-up with a dentist for
complete diagnosis and long-term care. Long-term sequelae can include pulp death,
root resorption, and displacement or developmental defects of permanent tooth successors.
Trauma to the teeth is not life threatening; however, associated maxillofacial injuries
and fractures can compromise the airway. Morbidity to the teeth may be individualized
to primary and permanent teeth. Fractures are more common in permanent teeth; primary
teeth usually become displaced.
Primary teeth - Failure to continue eruption, colour changes, infection, abscess,
loss of space in the dental arch, ankylosis, injury to the permanent teeth, abnormal
exfoliation.
Permanent teeth - Colour changes, infection, abscess, loss of space in the dental
arch, ankylosis, resorption of root structure, abnormal root development.
Sex
The male-to-female ratio is 2-3:1.
Age
The average age of injury is variable. In youths, falls and sporting activities
account for most injuries. In later teenaged years, road traffic accidents (RTA)
account for most injuries.
A complete medical history including a detailed account of the trauma/accident which
resulted in the tooth/teeth injury should be recorded. Following which the clinical
recording of the injury is done.
Different physical and clinical findings present depending on where the tooth is
fractured. Note the fracture's extent and the patient's age. The Ellis classification
has been designed for evident fractures.
Ellis Class I fractures involve only the enamel; these injuries may show minor chipping
with rough edges.
Ellis Class II fractures involve enamel and dentin; patients may complain of pain
to touch and sensitivity to air. Patients younger than 12 years have immature teeth
with much less dentin spanning the space between the pulp and enamel. The chance
of infection and damage to the pulp in this age group is much greater.
Ellis Class III fractures involve enamel, dentin, and pulp. Patients complain of
pain with manipulation, air, and temperature. Pinkish or reddish markings around
surrounding dentin or blood in the centre of the tooth from the exposed pulp may
be present.
Root fractures are clinically difficult to diagnose; patients may notice abnormal
mobility and sensitivity to percussion of the tooth.
Dentoalveolar fractures may cause patients to complain of malocclusion and mobility
with findings of a mobile group of teeth.
Treatment options for an enamel-dentin crown fracture with pulpal exposure in the
primary dentition include: Direct pulp capping, Cvek pulpotomy, cervical-depth pulpotomy,
pulpectomy or extraction.
The indication for a partial (Cvek) pulpotomy is a small and recent pulpal exposure
less than 2 weeks old.
Indications for a deep cervical pulpotomy include: A large pulpal exposure, pulpal
exposures older than 2 weeks, or if hemostasis cannot be obtained during a Cvek
pulpotomy procedure.
When the trauma has resulted in chronic inflammation or necrosis of the pulp, a
pulpectomy should be considered.
Permanent Tooth
Treatment for a case of enamel infraction consists of sealing the cracks – using
any enamel adhesive system.
For an Ellis Class I dental fracture, dental care involves removing the sharp edges
to prevent injury to the soft tissues of the mouth. Alternatively, the fracture
may be restored with composite material.
For an Ellis Class II fracture, the dentin should be coated with a protective covering–
as an interim measure. Allow up to 8 weeks for the injured tooth to recover before
placing the final composite restoration.
For an Ellis Class III complex fracture of the permanent tooth with incomplete root
formation: the main goal is to retain a viable dental pulp, and permit completion
of root growth. Therefore, if the pulp exposure is very recent or very small, a
direct pulp cap may be performed. For an exposure larger than 2mm, a Cvek pulpotomy
may be performed, removing only a millimetre or two of infected pulp tissue. For
an exposure older than two hours, a cervical-depth pulpotomy may be needed – ideally
using only saline irrigation to achieve haemostasis.
For an Ellis Class III in permanent teeth with complete root formation, root canal
treatment is advised.
Luxation, Lateral displacement, Extrusion
A. Diagnosis
Luxation involves displacement of a tooth in a labial, lingual, or lateral direction.
If the displacement is less than 5 mm, the dental pulp will remain vital in about
50% of the cases.
Lateral luxation is an angular displacement of the tooth while it remains within
the socket. There is usually an associated fracture of the supporting alveolar bone,
especially with labial and palatal luxations.
An extrusion occurs when a tooth is only partially removed from the socket.
In the primary dentition, the alveolar bone surrounding the tooth is relatively
elastic, so the most common injury in toddlers is a dental luxation (displacement
injury) – with gingival hemorrhage.
B. Management
I. Primary Tooth
A primary tooth with a luxation in the labial direction needs to be extracted, to
avoid further damage to the developing permanent tooth bud.
In other cases, however, it is possible to splint the luxated primary tooth back
into normal position using resin-modified glass ionomer cement. The cement is mixed
fairly thick, and placed on the labial and lingual surfaces of the luxated tooth
– and a few adjacent teeth. The luxated tooth is held in the ideal position while
the cement is setting. The splint is removed after 10 days.
II. Permanent Tooth
For any severe luxation injury: an anti-inflammatory agent, an analgesic and an
antibiotic are prescribed.
For a lateral luxation, treatment includes: repositioning after local anesthesia,
and applying a semi-rigid splint for 2-3 weeks. A post-treatment radiograph should
be performed to assure proper position of the tooth in the socket.
For an extrusive luxation, treatment includes: immediate repositioning and placement
of a semirigid (flexible) splint for 7-14 days.
III. Subluxation/ Dental Concussion (tooth was hit)
A. Diagnosis
Concussion results in mild injury to the periodontal ligament without tooth mobility
or displacement. Subluxation causes significant injury to the periodontal ligament,
resulting in some tooth mobility. There is usually bleeding at the marginal gingival
and the tooth is tender to percussion in subluxation.
B. Management:
I. Primary Tooth
Radiographs are taken to rule out root fractures. The child is then put on a soft
diet for a week, at the end of which a recall exam is performed.
II. Permanent Tooth
If the tooth is very mobile, and can be moved more than 2mm, a flexible wire and
composite splint may be placed for 7-10 days by periodic evaluation.
IV. Dental Intrusion (tooth was pushed in)
A. Diagnosis
An intrusion injury is the most severe type of luxation injury. The intruded tooth
is impacted into the alveolar bone, and the alveolar socket is fractured. The forces
that drive the tooth into the socket wall crush the periodontal ligament, and rupture
the blood and nerve supply to the teeth. The tooth may not be visible, and can be
mistaken for an avulsion.
Some studies have shown that intrusions of up to 3 mm have an excellent prognosis,
whereas the prognosis of incisors with severe intrusions (> 6mm) is hopeless. If
a permanent tooth is involved, radiographs may show an alveolar fracture, or tooth
displacement into the nasal cavity. Pulpal necrosis (death of the dental pulp) occurs
in 96% of cases of intruded permanent teeth.
If a primary incisor is involved in an intrusion injury, a lateral anterior radiograph
should be taken of the traumatized region to determine the proximity of the intruded
primary root tip to the developing adult tooth bud.
B. Management
I. Primary Tooth
Allow the primary tooth to spontaneously erupt over a 2 to 3 month period - as long
as the developing permanent tooth bud has not been injured. If re-eruption does
not begin within 2 months, extraction of the intruded primary tooth will be necessary.
A much intruded primary incisor, whose root tip is displaced into the developing
permanent tooth, should be extracted. Extraction of the intruded tooth will prevent
further damage or hypoplasia to the adult tooth bud.
II. Permanent Tooth
Current management strategies for intruded permanent incisors include: surgical
reduction (immediate repositioning), repositioning with traction (active repositioning),
and waiting for the tooth to return to it pre-injury position (passive repositioning).
Incisors intruded less than 3mm may be allowed to reposition themselves.
Incisors intruded between 3–6 mm are unpredictable, but they may be orthodontically
extruded within 3-6 weeks.
Incisors that have been intruded beyond 6 mm should be immediately repositioned
(surgically) to their normal position – followed by root canal treatment.
Root canal treatment is recommended in permanent teeth with complete root development.
If there is any doubt about pulp vitality, or if root resorption begins, then a
pulpectomy must be performed, followed by interim placement of intra-canal calcium
hydroxide. After apical closure and root health are confirmed, the canal is filled
with a standard root canal material (gutta percha).
Root fractures occur in only 7% of dental injuries. Horizontal root fractures occur
in anterior teeth, and are caused by direct trauma. Vertical root fractures usually
occur in molars, and may be caused by clenching or trauma to the mandible. Vertical
root fractures are more difficult to detect, and may not be found until extensive
tooth destruction has occurred.
A horizontal root fracture is classified based on the location of the fracture in
relation to the root tip (apex). Horizontal root fractures may occur in: the apical
third, middle third, or cervical third of the root. The prognosis worsens the further
cervically (towards the crown) the fracture has occurred. Tooth fractures are often
not apparent during a clinical examination, and can usually only be diagnosed using
appropriate radiographs. Radiographs with at least two views are required for making
this diagnosis.
B. Management
I. Primary Tooth
As long as no abscess or excessive mobility occurs, the primary tooth with a fractured
root can simply be monitored for health. If a portion of the root is abscessed or
extremely mobile, it can be extracted, and the remaining root fragment will resorb
normally. For coronal third fractures in primary teeth, the coronal third is extracted,
leaving the apical portion of the root to resorb normally. Do not “chase” apical
third fragments.
II. Permanent Tooth
The most important factor in the success and treatment of a horizontal root fracture
is the immediate reduction of the fractured segments, and complete immobilization
of the coronal segment. Root fractures must be diagnosed before the body tries to
“repair” the problem, and before the blood clot prevents apposition of the fractured
segments. If more than 24-72 hours have elapsed, it may be impossible to obtain
close apposition of the segments.
Treatment for horizontal root fractures consists of rigid fixation (immobilization)
in an attempt to get the cementum and dentin to heal. The tooth is splinted to the
adjacent normal teeth with a very rigid wire and composite splint for 8 weeks. Serial
radiographs are then taken at 6 month intervals after the splint is removed.
Sometimes extraction may be the only option; especially in vertical root fractures.
The alveolar bone, which supports the teeth, may experience a fracture at: the alveolar
socket wall, the alveolar process, or as a comminuted (shattered) fracture of the
supporting bone. Segmental fractures involve multiple teeth and their supporting
alveolar process.
B. Management
I. Primary Tooth
For any severe luxation injury: an anti-inflammatory agent , an analgesic , and
an antibiotic are prescribed.
Treatment of alveolar process fractures requires manually repositioning the segment
of displaced teeth back into proper arch alignment. A very rigid splint is applied
for two months.
II. Permanent Tooth
For any severe luxation injury: an anti-inflammatory agent, an analgesic , and an
antibiotic are prescribed.
Treatment of alveolar process fractures requires manually repositioning the segment
of displaced teeth back into proper arch alignment. A very rigid splint is applied
for two months.
Prevention of dental injuries
Dental injuries increase sixfold to eightfold when mouth protection is not used.
Education of athletes and coaches may encourage greater use of mouth guards. Educating
physicians and the public about first aid for dental injuries may reduce complications
later.
A dental avulsion occurs when a tooth is completely displaced or knocked out of
the dental socket. Dental avulsion injuries occur most frequently in children between
the ages of 7 and 9, an age when the alveolar bone surrounding the tooth is relatively
resilient. Adult teeth that are avulsed (knocked-out) should be considered for immediate
replantation in order to enhance the tooth’s long-term prognosis.
The best way to preserve a tooth that has been knocked out (avulsed) is to put it
back into its socket as quickly as possible. The single most important factor to
ensure a favourable outcome after replantation is the speed with which the tooth
is reimplanted. If immediate replantation isn't possible, the tooth should be placed
into a protective solution.
Avulsions are associated with poor post-treatment outcomes. Almost all replanted
teeth show replacement resorption and ankylosis – because immediate replantation
rarely happens. Replacement resorption leads to fusion of the tooth root with the
adjacent alveolar bone. In children who have not achieved skeletal maturity, replacement
resorption leads to progressive infraocclusion (the tooth appears unerupted) during
the adolescent growth spurt.
Every tooth has a protective layer surrounding the root, which is called the periodontal
ligament. The periodontal ligament is very sensitive, and will quickly dry out and
die - unless the tooth is immediately placed in a protective solution, such as milk
or saline. With every minute that the tooth is left out of the mouth to dry, more
cells in the periodontal ligament will die. After 15 minutes of dry storage, irreversible
damage to the periodontal cells (the root covering) occurs. If the cells of the
periodontal ligament are allowed to die, the child will eventually lose the tooth.
The goal of reimplanting the tooth into the socket is to preserve the health of
the tooth's outer periodontal ligament.
B. First Aid for an Avulsed Tooth
I. Primary Tooth
A primary tooth that has been avulsed is usually not reimplanted. The risk of injury
to the developing permanent tooth bud is high.
II. Permanent Tooth
Do not touch the root of the tooth. Handle the tooth by the crown only.
Rinse the tooth off only if there is dirt covering it. Do not scrub or scrape the
tooth.
Attempt to reimplant the tooth into the socket with gentle pressure and hold it
in position.
If unable to reimplant the tooth, place it in a protective transport solution, such
as Hank's solution, milk, or saline. This will hydrate and nourish the periodontal
ligament cells which are still attached to the root. A small container of Hank's
Balanced Salt Solution can be purchased in dental emergency kit form at many drug
stores.
The tooth should not be wrapped in tissue or cloth. The tooth should
never be allowed to dry.
Take the child to a dentist or hospital emergency room for evaluation and treatment.
Radiographs may need to be taken of the airway, stomach, and mouth if the tooth
cannot be found.
Tetanus prophylaxis should be considered if the dental socket is contaminated with
debris.
C. Management
I. Primary Tooth
The primary avulsed tooth is generally not reimplanted – to avoid injury to the
developing permanent tooth bud.
II. Permanent Tooth
Place the tooth in Hank's Balanced Salt Solution.
Take a medical and dental history, and perform a physical examination. Rule out
CNS injury.
Examine the orofacial area. Inspect the oral soft tissue for embedded tooth fragments,
lacerations, or ecchymosis (bruising). Palpate the teeth and dentoalveolar area
to check for mobility. Evaluate TMJ function.
If the tooth is missing, rule out aspiration or ingestion.
Take a maxillary occlusal radiograph, as well as a lateral anterior radiograph of
the injured area. Consider taking a panoramic radiograph to rule out condylar or
mandibular fractures.
Gently aspirate the injured area without entering the socket. If a clot is present,
dislodge and remove it using light saline irrigation. Do not curette the socket.
The tooth should be carefully held by the crown, and not by the root. The avulsed
tooth should be reintroduced into the dental socket slowly.
Tooth Reimplantation Guidelines
For a mature tooth with a closed apex: If the extra oral dry time is < 60 minutes,
re-implant as soon as possible. If the extra-oral dry time is>
60 minutes, soak
in citric acid or curette the root; then soak in stannous fluoride for 10 minutes.
Rinse with saline. Perform root canal therapy one week following the trauma.
For an immature tooth with an open apex: If the extra-oral dry time is < 60 minutes,
soak in doxycycline (1mg/20 ml saline) for 5 minutes. If the extra-oral dry time
is >60 minutes, provide the same treatment as for a closed apex.
Apply a flexible, functional splint for 7 to 10 days. If an alveolar fracture is
present, provide a very rigid splint for 4-6 weeks.
After re-implantation, gently compress the facial and lingual bony plates. Suture
any lacerations.
Provide antibiotic coverage for 10 days to prevent infection. Consider prescribing
tetracycline or penicillin.
Prescribe chlorhexidine gluconate rinses, and provide oral hygiene and diet instructions.
Provide analgesics to control pain. For children, consider prescribing acetaminophen
and codeine for mild to moderate pain. The dose is 15 mg/kg/dose of acetaminophen,
every 4 hours. Do not exceed 2.6 g/day of acetaminophen.
Arrange for tetanus vaccination if the wound was dirty, or if the vaccination requires
updating.
Follow-Up Care After 7 To 10 Days
For a tooth with an open apex, the goal is revascularization of the pulp. For a
tooth with an open apex and extra-oral dry time 60 minutes no endodontic treatment
is initially required. Re-evaluate every 3-4 weeks for pathosis. In case of pulp
pathosis, begin an apexification procedure.
For a tooth with an open apex and
extra-oral dry time >60 minutes: begin an apexification procedure.
For a tooth with a closed apex: provide traditional endodontic treatment and obturation.
This is done to prevent of eliminate toxins from entering the root canal space.
Remove the splint at this 7 to 10 day treatment visit.
Patients are recalled to the dental office every 3-4 weeks of sensitivity testing.
Thermal tests may be used.
Long-term follow-up is essential for 2 to 3 years after the re-implantation procedure.
Endodontic Obturation for Avulsed Teeth with Closed Apices
For a tooth with endodontic treatment started 7 to 10 days after avulsion, obturate
after 1 to 2 months of treatment with calcium hydroxide paste.
For a tooth with radiographic signs of resorption or pathosis, or for a tooth which
had endodontic treatment started more than 14 days after the avulsion, treat long
term with a dense mix of calcium hydroxide. The calcium hydroxide is changed about
every 3 months. Obturate when an intact lamina dura can be visualized.
Summary
Diagnosis
Definition
Presentation
Complications
Treatment
Reversible
Pulpitis
Pulpal
inflammation
Pain with hot, cold, or sweet stimuli
Periapical abscess, cellulitis
Filling
Irreversible Pulpitis
Pulpal inflammation
Spontaneous, poorly localized pain
Periapical abscess, cellulitis
RCT, extraction
Abscess
Localized bacterial infection
Localized pain and swelling
Cellulitis
I & D and RCT or extraction
Cellulitis
Diffuse soft tissue bacterial infection
Pain, erythema and swelling
Regional spread
Antibiotics and RCT or extraction
Pericoronitis
Inflamed gum over partially erupted tooth
Pain, erythema and swelling
Cellulitis
Irrigation, antibiotics if cellulitis also present
Tooth Fracture
Broken tooth
Clinical examination and radiography
Pulpitis and sequelae
Fillings, with or without RCT, extraction
Tooth Luxation
Loose tooth
Clinical examination and radiography
Aspiration, pulpitis and sequelae
Splinting, with or without RCT, extraction
Tooth Avulsion
Missing tooth
Clinical examination
Ankylosis, resorption
Re-implantation and splinting
Tooth Subluxation
Tooth was hit
Clinical examination and radiography
Pulpitis and sequelae
Splinting, periodic evaluation, RCT, extraction
Tooth Intrusion
Tooth is pushed in
Clinical examination and radiography
Pulpitis and sequelae
Periodic evaluation, repositioning, RCT
Root Fracture
Root is broken-vertical or horizontally
Clinical examination and radiography
Pulpitis and sequelae
RCT or extraction
Dentoalveloar Fracture
Fracture of supporting alveolar process
Clinical examination and radiography
Loss of teeth
Repositioning and splinting
RCT: Root Canal Treatment; I & D: Incision and Drainage.
Cookies help us to deliver our services. By using our services you agree to our use of cookies.